






Care Scarcity? Care Migration and Political Demography
October 29, 2020
Humanity has reached a particular global social situation in the 2010s. Since the 1980s there has been a rather unique interplay between aging, ongoing marketization with no increase in redistribution, and the death of the peasantry. These factors and their historical dynamic have led to care scarcity and a related dramatic increase in the care migration industry. These developments put the migrant caregivers into a very difficult position, especially with the ongoing COVID-19 pandemic making access to healthcare even more important globally. Huge chunks of the global population – and not only poor countries – are at the mercy of various care systems increasingly based on migrant labor. Meanwhile, migrant workers are caught in the crossfire between increasing demand for their work, increasing volatility in their employment, increasing hostility toward migrants, and increasing securitization also due to the pandemic. We have reached a point where care for the sick and elderly is becoming more competitive and very fragile.
Increasing domestic and healthcare migration
We lack systematic global data for domestic and healthcare workers. For 2015, the International Labour Organization (ILO) estimated that there were around 67.1 million domestic workers, of whom 11.5 million were migrants and almost three quarters were women. In the meantime healthcare migration has also gone up. An estimate of the World Health Organization (WHO) for 2013 showed a healthcare worker shortage of 17.4 million and projected a dramatic increase in demand that could only be met with increasing migration. The relatively rich OECD countries (United States excluded) have increased the stock of foreign-trained nurses between 2007 and 2016 by at least 80% and the number of such doctors by at least 45%. By 2016, the number of foreign-trained doctors in the above countries reached almost half a million, while the number of foreign-trained nurses is well above 300,000. Rates of foreign-born doctors have gone up by at least 10 percentage points in some countries, reaching 40% or 50% of all doctors (many of whom were blocked in their movement during the COVID-19 pandemic due to local and national lockdowns).
Aging, rising health costs, and unchanging redistribution
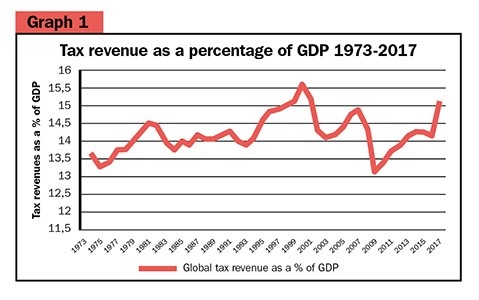
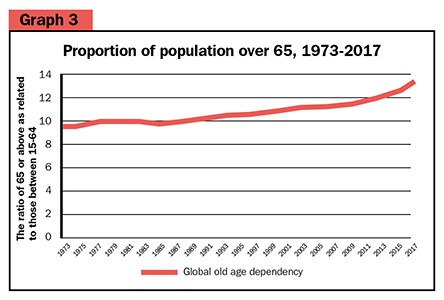
The rapidly aging population and the care of elderly dependents put significant burdens on the younger generations both in terms of labor productivity and actual care needs. This is especially the case given the extended global stagnation of state redistribution, as noted by József Böröcz (2016) in his study on work-related social contribution. Furthermore, the share of tax revenues (redistribution rates) in the Gross Domestic Product (GDP) has also stagnated globally, oscillating around 14% on average according to World Bank figures (see Graph 1). At the same time, per capita health expenditure has been increasing at least since the 2000s at a higher rate than GDP per capita growth (see Graph 2). Globally, old age dependency has increased from 9.5% to 13.2% over this same period (see Graph 3). This includes countries still with a very young population as opposed to a very old Europe.
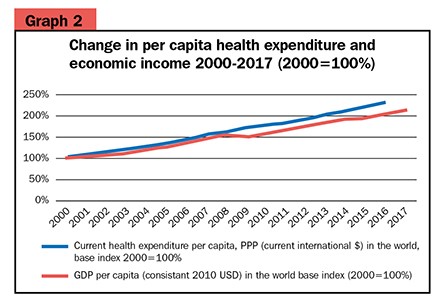
Until 2010, the world’s population aged at a slower pace than the growth of GDP per capita, meaning that, despite the stability of redistribution rates, there were expanding resources available for public and market costs of old-age care. From 2010 onwards, however, the growth of old-age dependency ratios has been faster than the growth of the economy. This means that the income needed for per capita health expenditure can come from extra private sources (purchasing an increasing share of such services in the market using our own income) and/or the proportion of health-related public spending is increasing at the expense of other public goals. This reorganization, in turn, necessarily leads to an increase in market and welfare competition for social and health goods, making it even more difficult for care migrants also looking for social protection for themselves.
This set of problems can further complicate migration in several ways. Migrants may seek to purchase welfare services from their wages and remittances or to enter the welfare systems of the migration destination countries. Otherwise hostile states with well-established welfare systems can simultaneously penalize migrants and seek their social contributions in order to improve the taxation balance between aging, social and health needs, and public spending. Furthermore, in this social environment there are clear signs of competition not only among local groups and between local groups and migrants, but also among migrant groups themselves as evidenced by interviews with East European care workers rejecting the “costly” protection of incoming refugees. The COVID-19 pandemic has only increased these tensions and we have not yet seen the end of the current economic crisis.
Global care competition and state protection
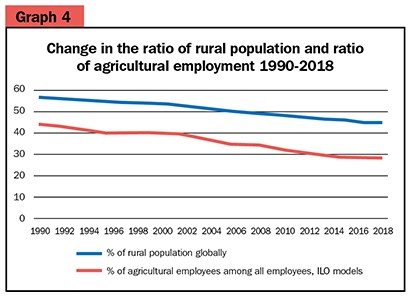
Such contradictions may become particularly acute due to changes in the level of state redistribution and aging rates after what Hobsbawm in The Age of Extremes called the “death of the peasantry.” The decline in agricultural employment in the mid-twentieth century continued at a rapid pace and fell below 30% globally by 2018; the rural population has become a minority compared to the urban population for the first time in history. This means that the care burdens associated with aging must be increasingly channeled into market and state redistributive systems as opposed to the historically important rural family-based systems. This means a decreasing weight for old-age care based on familial services. Even in poorer countries, the direct provision of food and material goods to the elderly within the family has declined as opposed to the need to purchase state and market health and social services, including those offered by local or immigrant elder-care givers. This shift is one of the most significant recent transformations in human history and has become a decisive moment in the age of globalization (Graph 4).
This means that marketization is going to lead to further marketization and related counter-demand for state protection, which is an ideal mix for authoritarian nationalisms. Therefore, we can conclude that contradictions around care scarcity in the current capitalistic economic order can be a source of transformation. Thus, during and post-COVID, political demographic debates will heighten, in which universal social protection and a radical change of the economic system will be seen as alternatives to contradictory marketization. And rightly so.
Attila Melegh, Corvinus University of Budapest, Hungary <attila.melegh@uni-corvinus.hu>


